Introduction
The PectusConnectUs method is a non-surgical approach – combining bracing, vacuum bell therapy, and specialized training – for treating Pectus Excavatum, Pectus Carinatum, Pectus Arcuatum, and other mixed chest wall deformities.
Since 2020, I’ve explored everything available – from medical literature to personal stories – while engaging in forums, speaking with patients, and analyzing countless images and videos to develop and refine this method.
It serves as an alternative to surgical options (such as the Nuss or Ravitch procedures) for those who prefer a non-invasive path.
This method builds on two original techniques from the 1970s, but I’ve taken them much further. I invented my own type of braces, redesigned the vacuum bell, and created a tailored training plan — combining proven principles with modern innovation for the best possible outcome.
Basic concepts

The concept is straightforward: just as dental braces and spinal corsets use consistent force to gradually reshape the body, chest braces and vacuum bells work the same way.
Wolff’s Law, by Dr. Julius Wolff (1836–1902), explains that bone adapts to repeated pressure. When force is applied over time, bones reshape and strengthen to better handle that pressure.
Davis’s Law, by Dr. Henry Gassett Davis (1807–1896), applies the same idea to soft tissues like ligaments, tendons, and fascia. With constant tension, these tissues gradually lengthen; if left loose, they shorten.
Chest braces and vacuum bells both use these principles. Braces apply external pressure to guide the chest wall, while vacuum bells create internal pressure (suction) to gently lift the sternum. Over time, the bones and soft tissue adapt and hold the new shape.
We’ve seen these principles at work for centuries. Kayan women in Asia and Ndebele women in Africa wore neck rings to elongate their necks. Their bones and tissues gradually lengthened—exactly as Wolff’s and Davis’s laws describe.

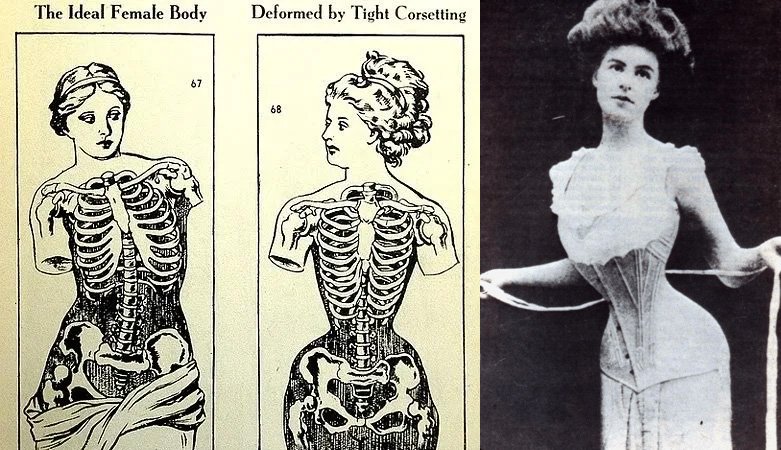
We’ve seen these principles at work in Europe as well. For centuries, women wore tight corsets to achieve an hourglass figure. Their ribs compressed, spines curved, and organs shifted — exactly as Wolff’s and Davis’s laws describe — all driven by beauty, not health.
History of the original methods
The Invention of Bracing for Chest Deformities
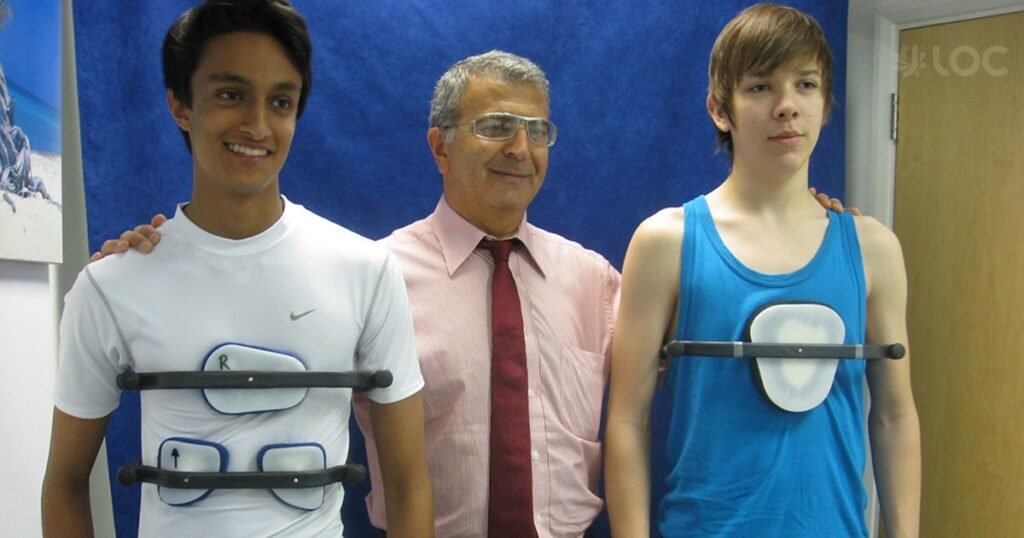
Dr. Sydney Abrao Haje (1952–2012) was a Brazilian orthopedist who pioneered the use of braces to treat Pectus Carinatum and Pectus Excavatum. In 1977, he developed the Dynamic Remodeling Method, treating nearly 5,000 patients during his lifetime. His work is continued by his son, Dr. Davi P. Haje, and supported by several published studies.
“Therapeutic forces regularly applied to deformed bones and cartilage can gradually reshape them in a corrective direction—especially in the flexible anterior chest wall.”
– Sydney A. Haje
Patients were typically instructed to wear the brace 23 hours a day, at least 5 days a week, along with specific exercises.
Dr. Haje’s first success came in 1977, treating a Pectus Carinatum patient with a custom-made brace that applied pressure to the protrusion. Over time, the chest wall flattened and the deformity corrected.
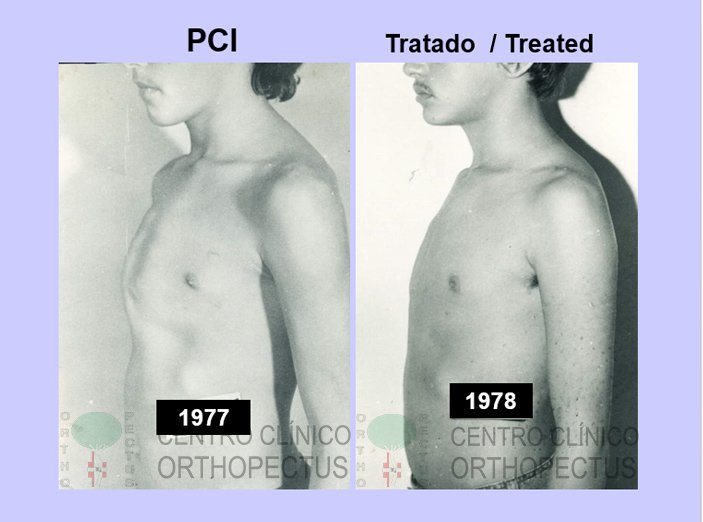
Ten years later, he applied the same method to Pectus Excavatum, this time focusing on the lower ribs. Pressure from the brace, combined with exercises that increase intrathoracic pressure, helped elevate the sternum while the lower ribs shifted inward—restoring the chest’s natural shape.
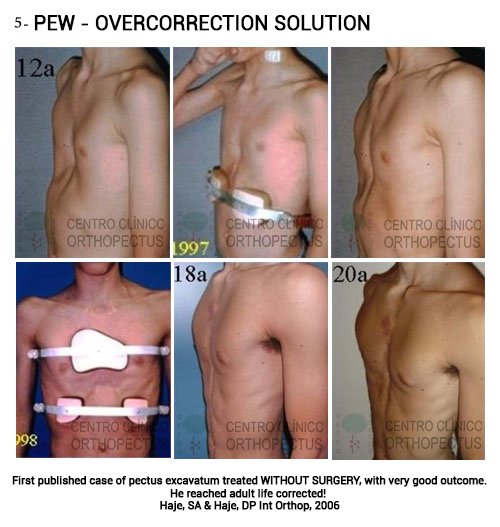
Over time, Haje found that starting with two braces often prevented overcorrection, which could cause a switch from Carinatum to Excavatum.
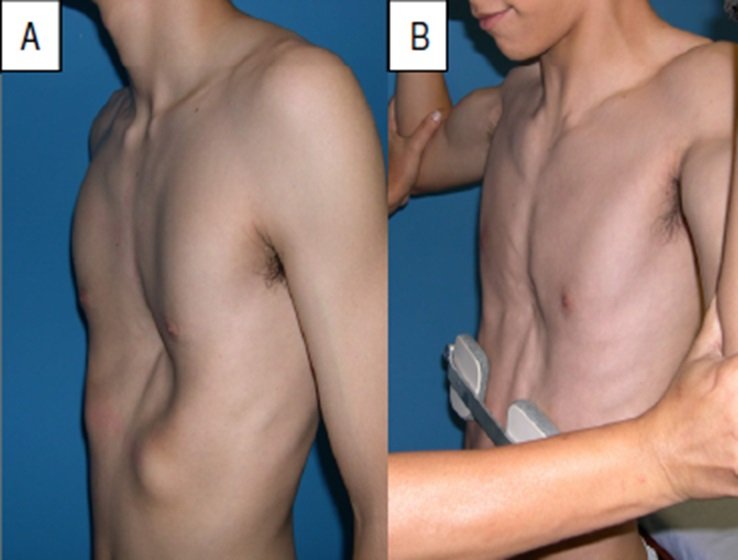
The flexibility test, developed by Dr. Sydney Haje, assesses how the chest wall responds to correction.
In image A, the patient is relaxed, showing the natural pectus excavatum depth. In image B, a deep breath is taken while gentle pressure is applied to the lower ribs, lifting the sternum by several centimeters—almost to normal contour.
Such flexibility suggests excellent potential for correction with bracing, exercises, and other non-surgical methods. Even if the chest is less flexible at first, targeted stretching, posture work, and vacuum bell use can gradually improve it.
When patients followed the protocol strictly, the success rate exceeded 93%.
However, compliance was a major issue. The brace was large, metallic, and bulky, designed to be worn outside of clothing, making it highly visible. Many patients were reluctant to wear it in public, which led to inconsistent use.
Social discomfort became the biggest barrier to success—more so than physical discomfort or trouble sleeping. Others eventually dropped out due to a loss of motivation or discipline.
The Invention of Vacuum Bells for Chest Deformities

In the early 1970s, Dr. Lewis Spitz (pediatric surgeon) and Dr. Fritz Lange (orthopedic surgeon) experimented with vacuum bell jars to lift sunken sternums. However, the glass material was heavy, uncomfortable, and kept patients confined to bed. As a result, these early attempts failed.
In the 1990s, Eckart Klobe, a German chemical engineer (born 1956), revived the idea using new materials. Many believe he used silicone vacuum bells—but that’s incorrect. Klobe actually used a rigid foam bell, molded directly onto his chest, connected to a vacuum cleaner via a hose and pressure gauge.
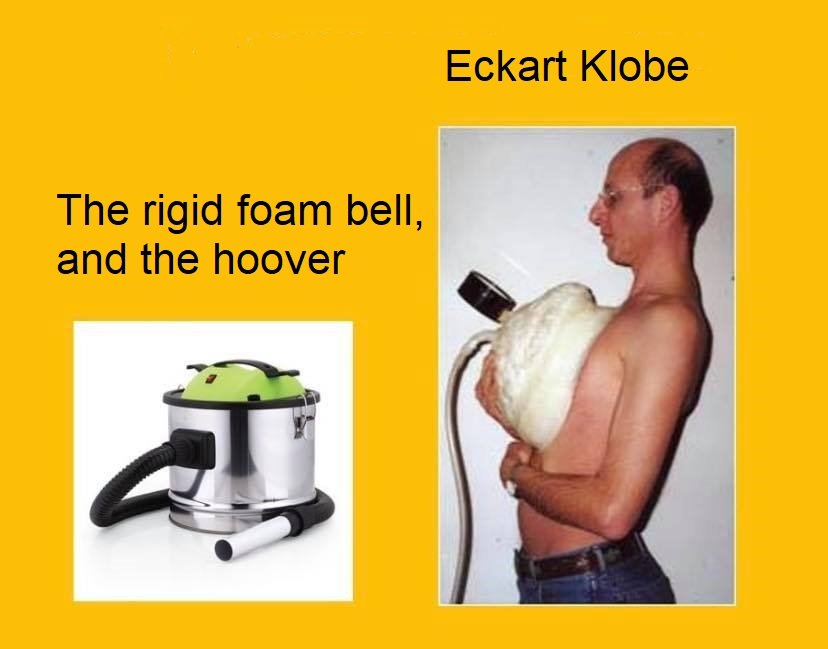
In a video clip, Klobe demonstrates that his sternum is elevated, with no fluid build-up under the skin.
By the early 2000s, Klobe introduced the now well-known white acrylic vacuum bells, which gained popularity—likely due to strong marketing and the temporary lift they provide. The device elevates the sternum immediately, but it usually sinks back after a few hours.
Vacuum bells can work like braces by slowly changing the shape of the chest—if they’re used the right way. Klobe had results using a large, hard vacuum bell made of polyurethane foam. It kept its shape and pulled only on the sternum, which is the area that needs to move.

The soft silicone vacuum bells with acrylic tops, which became popular later, are not what Klobe used in his own treatment. These softer bells spread out across the chest with every pump, pulling on areas they shouldn’t—like the nipples, stomach area, collarbones, and even the neck. This can cause pain, discomfort, and issues with blood flow or pressure. In some cases, pulling on the nipples may lead to gynecomastia (the development of breast tissue in males).
So even though vacuum bells can work based on proven medical principles, their design, fit, and how they’re used make a big difference in whether they help or cause problems.
The Birth of PectusConnectUs
Before 2020, I had only read online forums claiming that nothing works except surgery. After a failed Nuss surgery that left me in pain and without results, I couldn’t accept that there were no alternatives, so I began searching for other solutions. Sleepless nights led me to discover Dr. Sydney Haje’s bracing method and Eckart Klobe’s vacuum bell, along with other approaches. While both had potential, I quickly noticed their serious flaws—from bulky, visible braces that discouraged wear, to vacuum bells that only targeted the sternum and ignored posture, rib flare, and muscle imbalances.
I realized that neither method worked well enough on its own. So I merged their strengths:
-
A discreet brace, wearable in public and hidden under clothing, yet just as effective as the original metallic design.
-
The original hard, metallic brace—still made by me—for cases where maximum correction is needed.
-
A powerful, well-fitting vacuum bell that targets the right areas.
-
A complete training program with stretching, breathing, and strengthening to address both bones and soft tissues.
-
Coaching, progress tracking, and monthly photos to ensure proper progress and avoid overcorrection.
This combination—brace (soft & hard) + vacuum bell + targeted training + supervision—creates a synergistic effect, delivering results faster and more safely than any single method alone. That’s how the PectusConnectUs Method was born.
Today – Bringing PectusConnectUs to Life
In 2020, I had identified the problems and found a solution—but it needed to be brought to real life. Over the next three years, I developed the devices and the training program, refining every detail. By 2023, I worked with my first client, testing and improving the devices through a development process. After many iterations, the final versions of the devices were completed by the end of 2023.
In early 2024, my first client—a 36-year-old male with asymmetric Pectus Excavatum—successfully overcame his chest deformity. Throughout 2024, I welcomed many new clients of different ages and chest deformities from all over the world. Those who followed the PectusConnectUs methodology have improved their chest appearance and are on their way to becoming healthy.
In the following video, you’ll discover more about my method, the deep-rooted issues I’ve uncovered, and see plenty of examples, real footage from clients’ progress, and much more.
How it works?
The core of my method is bracing, and I will explain you why.
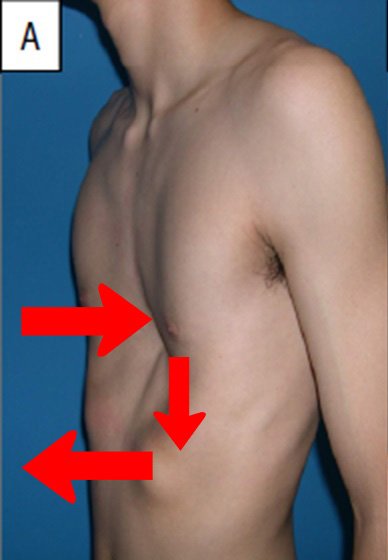
This image shows a person with pectus excavatum before treatment. The arrows show how the forces in the chest are working in the wrong way:
-
Incorrect breathing pattern: Instead of breathing with the diaphragm, the belly pushes outward and the lower ribs flare up with every breath.
-
Diaphragm not working properly: The diaphragm sinks lower and lower, which pushes the lower ribs outward even more.
-
Sternum caves in: Because of this abnormal breathing pattern, a vacuum forms inside the chest, pulling the breastbone (sternum) backward.
👉 The important point: the sunken sternum is not the main cause, but rather the result of this bad breathing and rib movement.
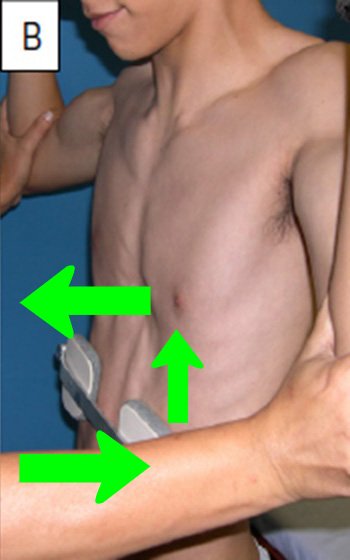
Here the same person is wearing a lower rib brace and practicing deep, correct breathing. The arrows now show how the forces have changed:
-
Correct breathing pattern: The brace gently pushes the lower ribs inward, which forces the diaphragm to work properly during breathing.
-
Diaphragm working correctly: The diaphragm now moves as it should, which increases the pressure inside the chest cavity.
-
Sternum elevates: With the ribs and diaphragm corrected, the breastbone naturally moves outward, reducing the sunken appearance.
👉 The key idea: the brace and breathing exercises don’t just push the sternum out — they correct the underlying breathing mechanics. Once the forces are balanced, the sternum rises as a natural consequence.
With time, the sternum (breastbone) and ribcage naturally remodel into a more healthier shape.
In other words, the brace doesn’t just push on the chest from the outside — it reprograms the way the chest and diaphragm work together. Once the breathing is corrected, the new forces inside the chest guide the sternum forward and keep it there.
The above mentioned Wolff’s Law and Davis’s Law apply here.
By combining the brace with corrected breathing, both the bones (sternum and ribs) and the soft tissues (cartilage, ligaments, diaphragm) respond to these natural laws. Over time, the chest wall doesn’t just shift temporarily — it remodels and stabilizes into a healthier shape.
The other main benefit of bracing is that it can be worn throughout the day (ideally 23 hours), keeping the chest wall under a guiding force most of the time. This high wear time is essential for achieving faster results. In my method, this is easy to accomplish: clients have an invisible “soft” brace they can use in public, and a “hard” brace—based on the original design—to wear at home and during training.
In contrast, vacuum bells can typically be worn only for a few hours a day.

The soft brace (left) and the hard brace (right) created by PectusConnectUs
Above bracing: Traning & Vacuum bell
Login page of the PectusConnectUs app
Now that you know bracing is the foundation of my method, it’s important to understand that it’s not the whole method.
Specialized training is just as essential. It’s a carefully designed program of strengthening, stretching, and breathing exercises, structured for the most effective results.
Training must always be performed while wearing the brace — together, they create a powerful synergistic effect.
Your personalized training will be delivered through my app, where you can follow interactive workouts, log your progress, upload photos, and chat directly with me.
An interactive workout in the app, with instructions and video demonstration
The vacuum bell is a fantastic tool — it softens the chest wall, makes it more flexible, and can drastically shorten treatment time. When it’s high quality and used correctly, it can even cut the treatment time in half.
But it’s important to understand: the vacuum bell is not the core of my method. In fact, I believe it’s often misused.
I’ve been contacted by many people who bought a standard vacuum bell, only to see their chest deformity get visibly and measurably worse. This really happens — not because the vacuum bell itself is harmful, but because it was used incorrectly. And ultimately, the problem lies with sellers who market it as a stand-alone, “ultimate” solution.
So why does this happen?
The vacuum bell lifts the sternum, but if you don’t address breathing patterns and the other root problems, the intrathoracic pressure remains unchanged. The elevation simply stretches the surrounding muscles, tendons, and cartilage — leaving the chest softer, but unstable.
That softness is a double-edged sword. Used correctly — as part of my full method — it’s an incredible advantage that speeds up results.
But used alone, without proper guidance, it can easily make the condition worse.
